
Knowledge, awareness, and practice of forensic odontology among dental surgeons in Bhubaneswar, India

Abstract
Aim: The aim of the study was to evaluate knowledge, awareness, and practice related to forensic odontology among dental surgeons in Bhubaneswar, East India.
Methods: A blind cross-sectional study, using a questionnaire with close-ended questions, was carried out. Interns were included to assess their knowledge and practice (related to dental record keeping) while in an institutional setting. In addition, dentists with Bachelor of Dental Surgery (BDS) and Master of Dental Surgery (MDS) qualifications (irrespective of their specialty) were assessed, which included purely private practitioners, purely academicians (dental surgeons teaching in dental colleges), and academicians-cum-practitioners.
Results: The total forensic odontology knowledge, awareness, and practice score (based on summing all the positive responses -- for all the relevant questions -- and calculating the percentage) was 80%, 76%, and 84% for the MDS, BDS, and intern group, respectively.
Conclusion: This study is the first of its kind to be undertaken in East India. The results show that there is an adequate level of knowledge and awareness regarding forensic odontology in all the groups investigated. Overall, the three groups also had adequate levels of good practice related to dental record keeping. However, regarding individual questions, there were some instances among the groups of inadequate levels of good practice.
Keywords
Introduction
Forensic science applies science and technology to the detection and investigation of crimes and the administration of justice. It has gained worldwide acclaim as an empowering field for using science in legal proceedings.[1] Forensic odontology is a branch of forensic science that focuses largely on the teeth and involves assisting in the identification of deceased individuals and criminals.[2] According to the Fédération Dentaire Internationale, forensic odontology is a branch of dentistry that deals with the proper handling of dental evidence in the interest of justice and with the proper evaluation and presentation of dental findings.[3] The main focus is to identify deceased individuals by comparing ante-mortem and post-mortem records.[4]
Dental identification has been a vital tool for identifying deceased individuals since 66 AD.[5] The first case of identification known to involve dentition in India occurred when Raja Jayachandra Rathore of Canouj died on the battlefield in 1191 and his body was identified by his prosthetic anterior teeth.[6]
Currently, the dearth of trained personnel, paucity of training facilities, inadequate introduction to the subject during undergraduate years, are the major hurdles in the expansion of the use of forensic odontology for the day-to-day benefit of society.[7] Although the Indian Dental Association[8] recommends that an individual’s dental records (radiographs, models, photographs, and clinical correspondence) should be securely retained for at least the legal minimum period of 5-6 years, the practice is yet to be enforced in all dental practices across India.[8]
Even the Indian Bachelor of Dental Surgery (BDS) curriculum, which is approved by the Dental Council of India, has only incorporated Forensic Odontology since 2007 (as a single chapter for third year students).[3] Further, the curriculum of the Indian master’s program [Master of Dental Surgery (MDS)] delegates the topic to the subjects of Oral Pathology and Microbiology and a preview for branches such as Preventive & Community Dentistry & Oral Medicine and Radiology. This prevents the teaching of Forensic Odontology alongside other specialism such as Conservative Dentistry & Endodontics, Orthodontics, Oral & Maxillofacial Surgery, Prosthodontics, Pedodontics, and Periodontics. The resultant low levels of knowledge among dental surgeons (who have undergone BDS and MDS degrees) might be severely handicapping the use of ante-mortem records in legal cases.
A systematic review of recent cross-sectional studies regarding the levels of knowledge, awareness, and practical application of forensic odontology among dentists in India revealed inadequacy and considerable variation in the practice of forensic odontology among dentists.[9] Various other studies have been conducted over the last decade on knowledge and awareness of forensic odontology using validated questionnaires in Indian cities such as Chennai,[4,10] Pune,[11] Kanpur,[12,13] Ghaziabad,[14,15] Kashmir,[16] and the Delhi National Capital Region[17] (which are in northern, western, and southern India). Most of these studies provided evidence that there were inadequate levels of knowledge and awareness of forensic odontology among the respondents.
Accordingly, considering the importance of the topic, the aim of this survey was to assess the knowledge and practice of forensic odontology among dental practitioners (both those with BDS and MDS qualifications) and interns in Bhubaneswar, in India. Interns were included in order to assess their knowledge and practice while in an institutional setting. Dentists with BDS and MDS qualifications (irrespective of their specialty), including purely private practitioners, purely academicians (i.e. dental surgeons teaching in dental colleges), and academicians-cum-practitioners, were treated as separate groups. The cross-sectional study used a blind questionnaire approach and is the first of its kind to be undertaken in East India.
Methods
Study design and sample
The cross-sectional study was conducted in July 2016 using a structured questionnaire with 25 close-ended questions in English. Survey validation was carried out using a pilot survey that involved 276 dental surgeons in Bhubaneswar, India, involving the following groups:
1. Dental surgeons (purely private practitioners, purely academicians, and academicians-cum-practitioners)
MDS (irrespective of their specialty): n = 74
BDS: n = 102
2. Interns: n = 100
Questionnaire
An overview of the 25 questions in the questionnaire is shown [Table 1] and the full questionnaire is shown in Supplementary Note 1. The data collected were used to evaluate the following components:
Questionnaire composition
| Category | Number of questions |
|---|---|
| Knowledge | 4 |
| Awareness | 3 |
| Practice | 17 |
| Source of knowledge | 1 |
| Total | 25 |
KNOWLEDGE, AWARENESS & PRACTICE QUESTIONNAIRE FOR FORENSIC ODONTOLOGY
| S. No. | QUESTIONS | YES | NO |
|---|---|---|---|
| 1 | Do you think forensic odontology is an important facade of dentistry? | ||
| 2 | Do you consider forensic odontology as an efficient method to identify victims in a mass disaster? | ||
| 3 | Do you consider bite marks pattern of human teeth as an important adjunct for assessing crime scene? | ||
| 4 | Do you think lip print patterns of human can be used for identification of a population? | ||
| 5 | Are you aware that you are eligible to appear in the court to present forensic dental evidence? | ||
| 6 | Are you aware of any methodology to estimate the dental age of an individual by examining the teeth which can be used for legal purposes? | ||
| 7 | Did your teaching curriculum include about maintaining dental records at institutional level? | ||
| 8 | Do you maintain dental records regularly? | ||
| 9 | Are you aware of the time period for which dental records should be maintained? | ||
| 10 | Do you use any pre-printed forms or electronic templates? | ||
| 11 | Do you record patients' basic personal details? | ||
| 12 | Do you record past medical and dental history? | ||
| 13 | Do you retain previous radiographs? | ||
| 14 | Do you retain dental casts? | ||
| 15 | Do you record full dental status on first visit? | ||
| 16 | Which tooth numbering system do you use? | ||
| 17 | Do you record common dental anomalies/unusual features? | ||
| 18 | Do you record basic details for restorative procedures? | ||
| 19 | Do you record basic details for denture/bridge work? | ||
| 20 | Do you record basic details for dental implant treatment? | ||
| 21 | Do you record basic identifying details on dental casts? | ||
| 22 | Do you record basic identifying details for intraoral digital and film radiographs? | ||
| 23 | Do you record basic identifying details for panoramic digital and film radiographs? | ||
| 24 | Do you use intraoral/extraoral photography in primary practice? | ||
| 25 | Do you keep printed/digital copy of photographs? |
1. Knowledge and awareness: regarding the significance of forensic odontology, dental records, dental age estimation, identification of an individual, bite marks, and acting as a court witness;
2. Practice: regarding maintenance of dental records and attitude towards maintenance of records;
3. Source of knowledge: regarding the presence of information on dental record maintenancein the curriculum (at the institutional level).
Questionnaire pre-testing and validation
A literature search was carried out and relevant questions/variables from previously validated questionnaires were used as the basis for our study hypotheses. Only questions/variables pertaining to knowledge and awareness about forensic odontology and practice related to dental records were selected (and, subsequently, a question on the source of the knowledge was added).
The questionnaire was piloted and validated for reliability. Closed-ended questions were used due to the resultant mutual exclusivity and easy preceding of the responses. In the pilot study, the questionnaire was self-administered by a convenience sample of 25 dental surgeons (who reflected the study population) and feedback was obtained on its overall acceptability in terms of its length, language clarity, and time requirements, and the feasibility for dentists to complete and return it. Based on the opinions, a mean content validity ratio (CVR) of 0.59 was calculated, using the formula CVR = [(E - (N/2))/(N/2)], where E is the number responses indicating “essential” and N is the total number of responses. This indicates high relevance but bias was also found. Therefore, the questionnaire was modified further before the survey was undertaken.
Statistical analysis
Descriptive statistics were used to summarize the responses to the questionnaire, with the results being presented as frequencies and percentages. Chi-square tests were used to compare the 3 groups, and the level of significance was set at P ≤ 0.05. The analysis focused on the “yes” responses in the three groups to the 25 questions (seven were related to knowledge and awareness, 17 were related to practice regarding dental record maintenance, and 1 was related to the source of knowledge). A frequency procedure was used to calculate the frequency of “yes” responses for the MDS, BDS, and intern groups.
In the final analysis, “yes” responses were given a score of 1 and “no” responses were given a score of 0; the scores were summed to obtain the overall scores in each group and they were then converted into percentages for (a) all the questions; (b) the knowledge and awareness questions; and (c) the practice questions. These percentages were classified into four levels: ≤ 50 (“poor”), 50-70 (“moderate”), 70-90 (“good”), and ≥ 90 (“very good”). The associations between the three percentages and the dental surgeon groups were studied using chi-square tests. In addition, the median scores were computed for between-group comparison.
The data were analyzed using Statistical Package for Social Sciences (SPSS) version 16.0 (SPSS Inc., Chicago, IL, USA).
Ethics approval
The study protocol was approved by the Institutional Review Board of the Faculty of Dental Sciences, Siksha ‘O’ Anusandhan University, Bhubaneswar. A blind survey approach was used and the questionnaire was distributed randomly, with all the relevant individuals who were willing to participate being asked to complete it. Blind surveys hide the sponsor or product of interest to reduce bias in the responses, thereby helping to increase the authenticity of the results.
Results
Knowledge
With respect to the first three questions on knowledge: (1) forensic odontology as an important area of dentistry; (2) forensic odontology as an efficient method to identify victims in a mass disaster; and (3) bite mark patterns of human teeth as an important adjunct for assessing crime scenes, > 90% respondents had adequate knowledge. Regarding the fourth question, about 78.3% of all respondents were aware that human lip print patterns can be used for individual identification. The highest proportion was observed for the MDS group (86.5%). The respective proportion in the BDS and intern groups was 77.5% and 73%, respectively. However, the association with the groups was not significant (P = 0.1).
Awareness
Only about 40% of the respondents were aware about the required time period for maintaining dental records, and surprisingly, the MDS group had the lowest level of awareness (24.3%). There was a significant between-group difference in the awareness level (P = 0.004). The awareness level in the BDS and intern groups was below satisfactory levels. About 72.1% of the respondents were aware of any methodology to estimate dental age that can be used for legal purposes. However, 83.8% of the MDS group were aware, but only 66.7% and 69% of the BDS and intern groups, respectively, were aware, and the association was significant (P = 0.030). Only 63.4% of respondents were aware that they were eligible to appear in the court to present forensic dental evidence, with no significant between-group difference (P = 0.461).
The results indicate that the levels of knowledge and awareness (with respect to the seven questions) need improvement irrespective of the dental surgeon group, as there were similar levels of knowledge and awareness between the 3 groups. Table 2 shows the proportions of positive responses to the 7 questions on knowledge and awareness for each of the 3 groups.
Demographic data about knowledge and awareness among all groups of dental surgeons, n (%)
| Questions | Response | Master in dental science (n = 74) | Bachelor in dental science (n = 102) | Interns (n = 100) | Total (n = 276) | χ2, P |
|---|---|---|---|---|---|---|
| Do you think forensic odontology is an important facade of dentistry? | Yes | 71 (95.9) | 98 (96.1) | 97 (97) | 266 (96.4) | χ2= 0.177, P = 0.916 |
| Do you consider forensic odontology as an efficient method to identify victims in a mass disaster? | Yes | 72 (97.3) | 92 (90.2) | 90 (90) | 254 (92.0) | χ2 = 3.828, P = 0.147 |
| Do you consider bite marks pattern of human teeth as an important adjunct for assessing crime scene? | Yes | 70 (94.6) | 92 (90.2) | 95 (95) | 257 (93.1) | χ2 = 2.163, P = 0.339 |
| Do you think lip print patterns of human can be used for identification of a population? | Yes | 64 (86.5) | 79 (77.5) | 73 (73) | 216 (78.3) | χ2 = 4.609, P = 0.100 |
| Are you aware that you are eligible to appear in the court to present forensic dental evidence? | Yes | 51 (68.9) | 61 (59.8) | 63 (63) | 175 (63.4) | χ2 = 1.547, P = 0.461 |
| Are you aware of any methodology to estimate the dental age of an individual by examining the teeth which can be used for legal purposes? | Yes | 62 (83.8) | 68 (66.7) | 69 (69) | 199 (72.1) | χ2 = 6.997, P = 0.030 |
| Are you aware of the time period for which dental records should be maintained? | Yes | 18 (24.3) | 43 (42.2) | 49 (49) | 110 (39.9) | χ2 = 11.16, P = 0.004 |
Practice
The level of practice also did not vary much among the three groups. Table 3 shows information on practice (regarding dental record maintenance) based on 17 questions.
Demographic data about practice of dental records among all groups of dental surgeons, n (%)
| Questions | Response | Master in dental science (n = 74) | Bachelor in dental science (n = 102) | Interns (n = 100) | Total (n = 276) | χ2, P |
|---|---|---|---|---|---|---|
| Do you maintain dental records regularly? | Yes | 53 (71.6) | 69 (67.6) | 80 (80) | 202 (73.2) | χ2 = 4.053, P = 0.132 |
| Do you use of pre-printed forms or electronic templates? | Yes | 42 (56.8) | 56 (54.9) | 57 (57) | 155 (56.2) | χ2 = 0.105, P = 0.949 |
| Do you record patients’ basic personal details? | Yes | 65 (87.8) | 83 (81.4) | 91 (91) | 239 (86.6) | χ2 = 4.166, P = 0.125 |
| Do you record past medical and dental history? | Yes | 71 (95.9) | 90 (88.2) | 95 (95) | 256 (92.8) | χ2 = 4.971, P = 0.083 |
| Do you record full dental status on first visit? | Yes | 69 (93.2) | 87 (85.3) | 90 (90) | 246 (89.1) | χ2 = 2.920, P = 0.232 |
| Do you retain previous radiographs? | Yes | 53 (71.6) | 76 (74.5) | 75 (75) | 204 (73.9) | χ2 = 0.282, P = 0.869 |
| Do you retain dental casts? | Yes | 37 (50.0) | 68 (66.7) | 68 (68) | 173 (62.7) | χ2 = 6.989, P = 0.030 |
| Do you use standard tooth numbering system? | Yes | 74 (100.0) | 101 (99.0) | 100 (100) | 275 (99.6) | χ2 = 1.712, P = 0.425 |
| Do you record common dental anomalies/ unusual features? | Yes | 73 (98.6) | 83 (81.4) | 93 (93) | 249 (90.2) | χ2 = 15.876, P = 0.000 |
| Do you record basic details for restorative procedures? | Yes | 59 (79.7) | 81 (79.4) | 84 (84) | 224 (81.2) | χ2 = 0.830, P = 0.660 |
| Do you record basic details for denture/ bridge work? | Yes | 59 (79.7) | 81 (79.4) | 84 (84) | 224 (81.2) | χ2 = 0.830, P = 0.660 |
| Do you record basic details for dental implant treatment? | Yes | 38 (51.4) | 79 (77.5) | 71 (71) | 188 (68.1) | χ2 = 14.052, P = 0.001 |
| Do you record basic identifying details on dental casts? | Yes | 36 (48.6) | 64 (62.7) | 78 (78) | 178 (64.7) | χ2 = 17.127, P = 0.000 |
| Do you record basic identifying details for intraoral digital and film radiographs? | Yes | 62 (83.8) | 86 (84.3) | 78 (78) | 226 (81.9) | χ2 = 1.603, P = 0.449 |
| Do you record basic identifying details for panoramic digital and film radiographs? | Yes | 62 (83.8) | 78 (76.5) | 70 (70) | 210 (76.1) | χ2 = 4.454, P = 0.108 |
| Do you use intraoral/extraoral photography in primary practice? | Yes | 61 (82.4) | 72 (70.6) | 87 (87) | 220 (79.7) | χ2 = 8.873, P = 0.012 |
| Do you keep printed/digital copy of photographs? | Yes | 41 (56.2) | 48 (47.1) | 58 (58) | 147 (53.5) | χ2 = 2.723, P = 0.256 |
With respect to eight of the questions, > 80% of respondents reported that they followed the correct practice. These questions were on the maintenance of records on the: (1) full dental status on the first visit; (2) patient’s basic personal details; (3) standard tooth numbering details; (4) medical and dental history; (5) common dental anomalies/unusual features; (6) basic details of restorative procedures; and (7) basic details of denture/bridge work. There was no significant between-group difference in the level of practice regarding these questions (P > 0.05).
With respect to four questions, 70-80% of respondents reported that they maintained the records. These questions were on: (1) regular maintenance of dental records; (2) retaining radiographs; (3) basic identifying details on panoramic digital and film radiographs; and (4) intraoral/extraoral photography in primary practice. Regarding the use of intraoral/extra oral photography in primary practice, the MDS group performed better than the other groups (P = 0.012).
With respect to five questions, only 50-70% of respondents reported practicing. These questions were related to: (1) using pre-printed forms or electronic templates; (2) retaining dental casts; (3) recording basic details on dental implant treatment; (4) recording basic identifying details on dental casts; and (5) keeping printed/digital copies of photographs. Regarding the questions on retaining dental casts, recording basic details on dental implant treatment, and recording basic identifying details on dental casts, the proportions were significantly different among the three groups.
Source of knowledge
About 75% respondents stated that their curriculum included information about the maintenance of dental records (at the institutional level). The percentage was almost the same in all three groups [Table 4].
Demographic data about teaching curriculum inclusion of maintenance of dental records among all groups of dental surgeons, n (%)
| Question | Response | Master in dental science (n = 74) | Bachelor in dental science (n = 102) | Interns (n = 99) | Total (n = 275) | χ2, P |
|---|---|---|---|---|---|---|
| Did your teaching curriculum include about maintaining dental records at institutional level? | Yes | 57 (77) | 77 (75.5) | 73 (73.7) | 207 (75.3) | χ2 = 0.250, P = 0.882 |
Overall percentage scores
To objectively assess the overall level of (a) knowledge, awareness, and practice; (b) knowledge and awareness; and (c) practice, the responses were converted into overall percentage scores and four corresponding levels (“very good,” etc.), which were assessed by group.
Figure 1 shows the distribution of the four levels related to overall knowledge and awareness and overall practice, respectively. The analysis of the overall percentage scores (for knowledge, awareness, and practice) is presented [Table 5].
Demographic data of total score analysis of knowledge, awareness and practice in all groups of dental surgeons, n (%)
| Category | Master in dental science (n = 74) | Bachelor in dental science (n = 102) | Interns (n = 100) | χ2, P |
|---|---|---|---|---|
| Total score | ||||
| ≤ 50 (low) | 4 (5.4) | 6 (5.9) | 9 (9) | χ2 = 22.331, P = 0.001 |
| 50-70 (average) | 15 (20.3) | 36 (35.3) | 16 (16) | |
| 70-90 (good) | 47 (63.5) | 38 (37.3) | 46 (46) | |
| ≥ 90 (very good) | 8 (10.8) | 22 (21.6) | 29 (29) | |
| Total | 74 (100.0) | 102 (100.0) | 100 (100) | |
| Median score | 80 | 76 | 84 | |
| Knowledge and awareness score | ||||
| ≤ 50 (low) | 1 (1.4) | 10 (9.8) | 5 (5) | χ2 = 10.635, P = 0.100 |
| 50-70 (average) | 11 (14.9) | 12 (11.8) | 19 (19) | |
| 70-90 (good) | 50 (67.6) | 69 (67.6) | 57 (57) | |
| ≥ 90 (very good) | 12 (16.2) | 11 (10.8) | 19 (19) | |
| Total | 74 (100.0) | 102 (100.0) | 100 (100) | |
| Median score | 85.71 | 71.43 | 78.57 | |
| Practice score | ||||
| ≤ 50 (low) | 5 (6.8) | 11 (10.8) | 9 (9) | χ2 = 19.538, P = 0.003 |
| 50-70 (average) | 14 (18.9) | 28 (27.5) | 14 (14) | |
| 70-90 (good) | 43 (58.1) | 35 (34.3) | 38 (38) | |
| ≥ 90 (very good) | 12 (16.2) | 28 (27.5) | 39 (39) | |
| Total | 74 (100.0) | 102 (100.0) | 100 (100) | |
| Median score | 76.47 | 76.47 | 88.24 | |
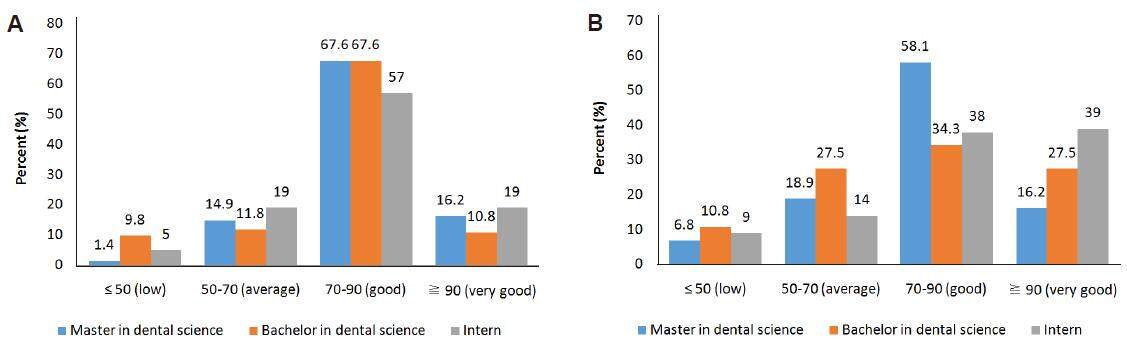
Figure 1. (A) Score analysis of knowledge and awareness in all groups of dental surgeons; (B) score analysis of practice of forensic odontology in all groups of dental surgeons
Regarding the overall knowledge, awareness, and practice percentage score, 63.5% of the 74 MDS respondents were categorized as “good” and 10.8% were “very good.” The “good” and “very good” together constituted 74.3%. Among the 102 BDS respondents, only 37.3% were “good” and 21.6% were “very good”. The “good” and “very good” together constituted 58.9%. Among the 100 interns, 46% were “good” and 29% were “very good.” There was a significant between-group difference in the total percentage score (P = 0.001).
In the MDS group, the levels of knowledge and awareness were either “good” or “very good” for 83.8% of respondents. The corresponding proportions in the BDS and intern groups were 78.4% and 76%, respectively. The levels of knowledge and awareness were either “poor” or “moderate” for 16.3% of MDS respondents, 21.6% of BDS respondents, and 24% of interns. There was no significant between-group difference in the overall knowledge and awareness percentage score (P = 0.1).
Discussion
Ante-mortem data in the form of dental records can be used as a vital tool for confirming or disproving identity. Relevant professional bodies, including the Indian Dental Association[8] and the Indian Association of Forensic Odontology[18] have been encouraging patient record maintenance for the period of time prescribed by the law. Irrespective of the mandated time period, many dental surgeons are still unaware of their duties regarding when their patient care responsibilities cease. A comparison of studies conducted in various cities in India showed that although there is adequate exposure to forensic odontology during undergraduate education, this exposure may not be sufficient to instill interest in or awareness of the kinds of dental records needed to support forensic work in legal cases. Moreover, the busy nature of dental practices is the biggest challenge associated with accurate and complete dental record keeping.
Regarding the international situation, according to Dental Board of Australia guidelines, forensic odontology is one of 13 registrable dental specialties. Furthermore, a survey of Australian dentists showed that the majority of undergraduate respondents recalled learning about forensic odontology during their education, but there was no exposure to this subject for postgraduates.[19] The reasons for making errors and barriers to accurate and complete record keeping included “lack of time” and “workload” associated with busy dental practices.[19] The need for record keeping guidelines in dental practices (from either the registration authority or a professional association) should be explicitly taken into account.[19]
In Brazil, law 5081/66 states[20] that dentists working in forensic dentistry can study each subject’s neck and head, rather than being limited to the dentition. Furthermore, the Brazilian Federal Council of Dentistry states that a patient’s dental record should contain professional data, the patient’s identification data, and data on self-reported medical history, the clinical examination, the treatment plan and any interruptions, prescriptions, and complementary tests.[20] However, a study in Brazil reported on unsatisfactory results associated with general dentists and forensic matters due to the sparse number of hours in undergraduate courses spent on forensic dentistry theory and practical skills along with the lack of teachers with expertise in the field.[20]
Delattre et al.[21] conducted a study to provide insight into the attitudes and practices of forensic dentists regarding ante-mortem dental records. The authors emphasized starting a dialogue among forensic dentists in order to develop standardized recommendations for the forensic dental community. Furthermore, a study based on guidelines set out in Article 9 of the patients’ rights law[21] for practitioners in Belgium found that young male dentists in large cities tended to use appropriate record keeping systems.[22] However, as the age of the dentists increased, the likelihood of completing dental records decreased.[22]
Avon et al.[23] studied the important factors in the field of forensics and highlighted another reason to maintain legible and legally acceptable records, that is, to assist legal authorities in the identification of victims and suspects. As described by Avon et al.,[23] Canadian dental schools devote several hours to forensic odontology during the last 2 undergraduate years by integrating the subject into oral pathology courses. The Bureau of Legal Dentistry at the University of British Colombia offers master’s and postdoctoral programs in forensic odontology. Furthermore, the American Academy of Forensic Sciences established the American Board of Forensic Odontology in 1976 and certifies dentists qualified in forensic odontology.[23]
Waleed et al.[24] compared the dental records kept by students in teaching hospitals with those kept by dentists in private clinics (focusing on elements that contribute to forensic identification with respect to American Academy of Pediatric Dentistry regulations). The study revealed that the students were more aware of the medico-legal purpose of dental record maintenance than the dentists.[24]
Regarding the situation in India, a 2016 survey by Navya and Raj[10] showed that general dental practitioners in Chennai have inadequate knowledge of and interest in forensic odontology, and these results are similar to those of a study by Preethi et al.[4] in 2011. The 5-year gap between the two studies clearly did not improve the situation in southern India, raising questions about the education system and the implementation of suggestions for improvement. A study of dental practitioners in Pune, reflecting the situation in western India, revealed inadequate clinical knowledge of forensic odontology, poor attitudes, and lack of good practice related to record keeping.[11] Moreover, a study[12] that included purely practitioners, purely academicians, and dentists with both roles showed that they had low levels of knowledge about the routine application of forensic odontology, indicating the need to further educate dental practitioners. Surprisingly, a study in Kanpur showed that practitioners had adequate levels of knowledge and good attitudes, but low levels of good practice regarding long-term dental record maintenance.[13]
This study is the first of its kind to be conducted in East India, and it provides evidence that there has been little change in the situation since other studies were conducted in India. The MDS group had the highest level of knowledge regarding forensic odontology, but the difference between the groups was not significant. A significant between-group difference in the level of awareness of the mandated time period for dental record maintenance was observed, with the MDS group being the worst group. This indicates that levels of knowledge and awareness need improvement irrespective of dental surgeon group. Furthermore, there was no between-group difference in the level of good practice.
The study has several limitations as per the sample size, answer bias, etc. Despite this, regarding the potential generalizability of the results, caution was exercised by ensuring that the survey respondents closely matched the demographic characteristics of the underlying population.
Sahni et al.[17] highlighted that success in acquiring extensive knowledge of forensic odontology would be more rational if there were better job opportunities in the field. Regarding record retention, regulations should be developed based on recommendations from professional bodies, and they should be implemented/inculcated into the system from the institutional level to the group/individual practices. In addition, quality control protocols would be useful to ensure accuracy and completeness regarding dental record maintenance for legal purposes. The up-to-date use of electronic patient files should be an integral part of dental record keeping. Forensically valued dental records should be maintained in detail, ensuring accuracy, legibility, and accessibility. Furthermore, profession-wide strategies for teaching students and professionals about forensic odontology should be implemented, including the provision of Continuing Dental Education modules by the Indian Association of Forensic Odontology.
In conclusion, dental records are created and maintained to contribute to the safety and continuity of dental care, for treatment decisions, treatment planning, and legal purposes. All three groups investigated had the basic knowledge required for good practice related to keeping dental records. Our result also showed adequate levels of knowledge and awareness regarding forensic odontology in all three groups. However, on individual correlation, the groups failed in practice related to particular questions, such as the mandated time period for maintaining dental records. Therefore, emphasis should be put on increasing knowledge at the grassroots level by developing better curriculums for undergraduates and postgraduates.
Authors’ contributions
The authors contributed equally to the study.
Financial support and sponsorship
None.
Conflicts of interest
The authors have no conflicts of interest and no financial disclosures.
Patient consent
Written informed consent was obtained fromthe respondents.
Ethics approval
The study protocol was reviewed and approved by the Institutional Review Board of the Faculty of Dental Sciences, Siksha ‘O’ Anusandhan University, Bhubaneswar.
REFERENCES
1. Quarino L, Brettell TA. Current issues in forensic science higher education. Anal Bioanal Chem 2009;394:1987-93.
3. Acharya AB, Sivapathasundharam B. Forensic odontology [J]. Shafer’s textbook of oral pathology. Fifth Edn. Elsevier: New Delhi; 2006. pp. 1199-227.
4. Preethi S, Eintein A, Sivapathasundaram B. Awareness of forensic odontology among dental practitioners in Chennai: a knowledge, attitude, practice study. J Forensic Dent Sci 2011;3:63-6.
5. Chandra Shekar BR, Reddy CV. Role of dentist in person identification. Indian J Dent Res 2009;20:356-60.
7. Iacopino AM. The influence of "new science" on dental education: current concepts, trends, and models for the future. J Dent Educ 2007;71:450-62.
8. Sharma A, Shokeen S, Arora R, Dhaginakatti SA. Survey on knowledge, attitude and practice of forensicodontology among private dental practitioners in Ghaziabad city, India. J Dent Specialitie 2015;3:43-7.
9. Gambhir RS, Singh G, Talwar PS, Gambhir J, Munjal V. Knowledge and awareness of forensic odontology among dentists in India: a systematic review. J Forensic Dent Sci 2016;8:2-6.
10. Navya N, Raj JD. To assess the knowledge and attitude toward forensic odontology among dentists in Chennai city. Int J Forensic Odontol 2016;1:17-20.
11. Harchandani N, Marathe S, Hebbale M, Ul Nisa S, Hiremutt D. Awareness of forensic odontology among general dental practitioners in Pune -- a cross-sectional study. J Adv Med Dent Scie Res 2014;2:10-6.
12. Khare P, Chandra S, Raj V, Verma P, Subha G, Khare A. Status offorensic odontology in metro and in tier 2 city in urban India. J Forensic Dent Sci 2013;5:134-7.
13. Nagarajappa R, Mehta M, Shukla N, Tuteja JS, Bhalla A. Awareness of Forensic Odontology among Dental Practitioners in Kanpur City, India: a kap study. J Dent Res Updates 2014;1:6-12.
14. Sharma A, Shokeen S, Arora R, Dhaginakatti SA. Survey on knowledge, attitude and practice forensic odontology among private dental practitioners in Ghaziabad city, India. J Dent Specialities 2015;3:43-7.
15. Sengupta S, Sharma V, Gupta V, Vij H, Vij R, Prabhat K. Forensic odontology as a victim identification tool in mass disasters: a feasibility study in the Indian scenario. J Forensic Dent Sci 2014;6:58-61.
16. Singh NN, Gowhar O, Ain TS, Sultan S. Exploring trends inforensicodontology. J Clin Diagn Res 2014;8:ZC28-30.
17. Sahni A, Rehani S, Mathias Y, Kardam P, Nagpal R, Kumari R. A questionnaire survey on forensic odontology: are we really aware? J Forensic Dent Sci 2016;8:113.
19. Al-AzriAR, Harford J, James H. Awareness of forensic odontology among dentists in Australia; are they keeping forensically valuable dental records? Aust Dent J 2015;61:102-8.
20. Nedel F, da Silva RHA, Lund RG, Nedel AP. Evaluation of identification cases involving forensic dentistry in the city of Pelotas, RS, Brazil, 2004-2006. Braz J Oral Sci 2009;8:55-8.
21. Delattre VF. Antemortem dental records: attitudes and practices of forensic dentists. J Forensic Sci 2007;52:420-2.
22. Dierickx A, Seyler M, de Valck E, Wijffels J, Willems G. Dental records: a Belgium study. J Forensic Odontostomatol 2006;24:22-31.
23. Avon SL. Forensic odontology: the roles and responsibilities of the dentist. J Can Dent Assoc 2004;70:453-8.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Rahman J, Routray S, Mishra SS, Mohanty I, Mohanty N, Sukla N. Knowledge, awareness, and practice of forensic odontology among dental surgeons in Bhubaneswar, India. J Unexplored Med Data 2017;2:26-33. http://dx.doi.org/10.20517/2572-8180.2017.01
AMA Style
Rahman J, Routray S, Mishra SS, Mohanty I, Mohanty N, Sukla N. Knowledge, awareness, and practice of forensic odontology among dental surgeons in Bhubaneswar, India. Journal of Unexplored Medical Data. 2017; 2: 26-33. http://dx.doi.org/10.20517/2572-8180.2017.01
Chicago/Turabian Style
Rahman, Juber, Samapika Routray, Sudhanshu S. Mishra, Ipsita Mohanty, Neeta Mohanty, Narayan Sukla. 2017. "Knowledge, awareness, and practice of forensic odontology among dental surgeons in Bhubaneswar, India" Journal of Unexplored Medical Data. 2: 26-33. http://dx.doi.org/10.20517/2572-8180.2017.01
ACS Style
Rahman, J.; Routray S.; Mishra SS.; Mohanty I.; Mohanty N.; Sukla N. Knowledge, awareness, and practice of forensic odontology among dental surgeons in Bhubaneswar, India. J. Unexplored. Med. Data. 2017, 2, 26-33. http://dx.doi.org/10.20517/2572-8180.2017.01
About This Article
Copyright

Data & Comments
Data


 Cite This Article 7 clicks
Cite This Article 7 clicks

 Like This Article 0
likes
Like This Article 0
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.