
Relationship between family function and low back pain in nurses working in a tertiary hospital in North Central Nigeria
 0
0Abstract
Aim: The study aimed to determine the relationship between family functioning and low back pain (LBP) in nurses in a tertiary hospital in North Central Nigeria.
Methods: A cross-sectional study using structured questionnaires was done among 204 randomly selected, eligible, consenting nurses in a tertiary hospital between August-November 2011. Sociodemographic data and Family APGAR Scores were collected, collated and analyzed with SPSS version 21.
Results: Results showed that 92.2% (188) were from high functioning families, while 7.8% had moderately dysfunctional families. None of the respondents were from severely dysfunctional families. Independent t-test did not show any significant difference in the family function scores for nurses with LBP and those that did not have LBP, t = 0.716, P = 0.475. Spearman’s rank correlation did not reveal any significant relationship between severity of back pain and Family APGAR. Spearman’s r = -0.046, P = 0.606.
Conclusion: Family function scores did not significantly differ for nurses with LBP and those without LBP. The low level of family functioning might have been due to the self-reported nature of the Family APGAR tool. Further studies should consider other assessments of family functionality as a possible predictor of LBP in nurses.
Keywords
Introduction
Work satisfaction and family support are psychosocial factors contributing to low back pain (LBP) in nurses.[1] Some researchers have reported that there is a connection between psychosocial factors, LBP and the resulting disabilities.[2,3]
Data is limited on the contribution of family functioning to LBP in nurses. A few studies have shown that LBP is influenced by low social support and poor social relationships outside the work environment, and this is supported by published data.[4]
Steel plant workers in South Africa, in a cross-sectional study by van Vuuren et al.[5] were found to have higher prevalence of LBP. This was related to shift work which in turn created additional demands on their family life. Long hours were reported to take up valuable family time, leading to decreased support from workers’ families, increase in their stress levels, and invariably predispose them to LBP.[5] This same South African study indicated that many workers came from dysfunctional families, but did not show any specific relationship with the prevalence of LBP. Responses to the family APGAR tool indicate perceived family social support but these are influenced by cultural differences which can play a significant role in one’s perception of family values.[5]
LBP is a form of pain, which is generally accepted to be an internal subjective experience that is neither easily observed by others nor quantified by measuring physiological markers or through bioassays. Pain assessment therefore heavily relies on self-reports. Pain research in humans has focused on testing and refining these self-reporting methodologies.[6-8] A better understanding of a patient’s perception of pain can be obtained leading to an understanding of the impact of pain on the biopsychosocial aspects of the patient’s life.[9] Quantifying pain provides a measure of assessing the effectiveness of treatment and helps when assessing the behavior of the patient’s pain. It provides a baseline from which to work and can be used to compare pain episodes.
The validity and reliability of various measures of pain have been extensively researched in Europe, America, and Asia.[10] In Africa on the other hand, very few studies have been conducted.[11] Most of the research into measurement of pain has been carried out using Anglo-American pain measures.[11,12] Assessment of back pain is made easier by using scales to measure the severity (intensity) of the pain. Pain scales are a convenient, easy and quick way of determining changes in the patient’s symptoms.[13]
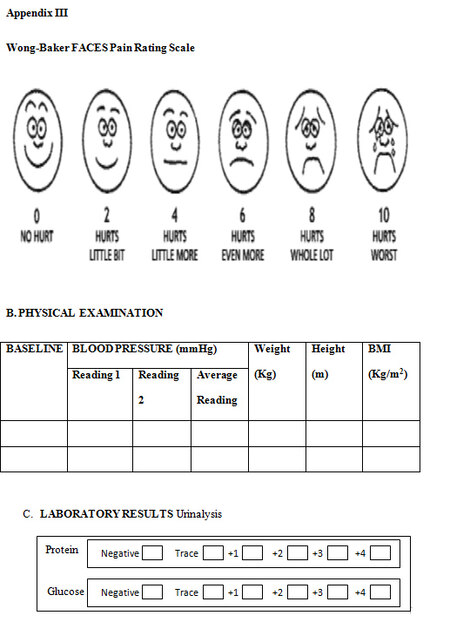
The Wong-Baker Faces (WBF) Pain Scale is easy to understand and can be used for children, adults and subjects with low educational levels.[14] Kim and Buschman[15] supported the appropriateness of using the WBF Pain Scale in older adults, to measure pain intensity. Their research also provided evidence on the usefulness of the WBF Pain Scale in cross-cultural settings. The WBF has been shown to be easy to administer, and sensitive to changes in pain after treatment.[16]
This paper endeavors to examine the relationship between family functioning and LBP in order to address factors outside the work place that may contribute to LBP in nurses.
Methods
A minimum sample size of 204 including a 2.5% non-response rate was determined based on the formula for estimating proportions, assuming 95% confidence interval and 80% power.[17] A cross-sectional hospital-based study was carried out with semi-structured questionnaires [Appendix I] administered to 204 randomly selected, eligible, consenting nurses. Eligible participants were selected by simple random sampling from a list of 489 full-time nurses obtained from the Director of Nursing Services. The semi-structured questionnaire was developed, reviewed by an expert jury consisting of an orthopedic surgeon, a family physician, a nurse and a physiotherapist. They were selected based on their participation in LBP management. These pre-tested questionnaires were then administered by the researchers to consenting, eligible nurses. Information was collected on socio-demographic factors including: the age, sex, religion and marital status; occupation and workload, family functioning and severity of back pain.

Appendix I
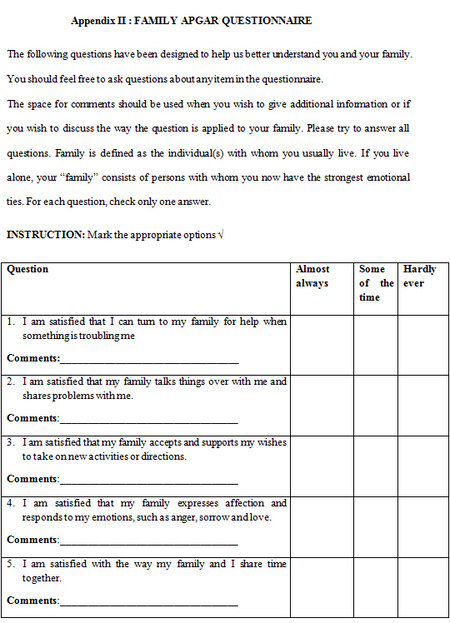
The family functioning was assessed with the family functioning tool-APGAR [Appendix II]. This tool consists of 5 parameters of family functioning: adaptability, partnership, growth, affection, and resolve. The acronym APGAR is comprised of the first letter of each parameter. The response options describe the frequency of feeling with each parameter on a 3-point scale ranging from (hardly ever) which is scored 0, to (almost always) which is scored 2. A total score in the range of 7 to 10 implies a highly functional family, a score of 4 to 6 implies a moderately dysfunctional family, while a score of 0 to 3 suggested a severely dysfunctional family.[5]
Appendix II
The severity of LBP was measured using the WBF Pain Scale [Appendix III]. A numeric value which ranged from “0-10” was marked by the respondents.[15] The scale also shows a series of faces ranging from a happy face which is graded as “0” meaning “no pain”, to a crying face at “10” which corresponds to “worst pain”. The individual chose the face that best described how they were feeling.[15]
Appendix III
Data was analyzed using SPSS version 21 Statistical Software (IBM Corp, NY, USA). Independent t-test was used to determine the relationship between family APGAR and LBP and Spearman’s correlation was used to determine the relationship between severity of back pain and family functioning. A confidence interval of 95% and a P value of less than 0.05 were considered significant.
Results
Socio-demographic characteristics of respondents
A total of 204 nurse respondents had valid questionnaires, 28 (13.7%) males, and 176 (86.3%) females. Their ages ranged from 22 to 53 years with mean age of 42.8 ± 8.5 years. They were mostly married (77.9%), and the majority (73.5%) had a duration of service > 10 years [Table 1]. Other details of this population had been previously published.[18]
Socio-demographic characteristics of respondents
| Variable | Frequency | Percentage |
|---|---|---|
| Gender | ||
| Male | 28 | 13.7 |
| Female | 176 | 86.3 |
| Age (years) | ||
| < 30 | 23 | 11.3 |
| 30-40 | 53 | 26.0 |
| 41-50 | 86 | 42.2 |
| > 51 | 42 | 20.5 |
| Marital status | ||
| Single | 31 | 15.2 |
| Married | 159 | 77.9 |
| Widowed | 14 | 6.9 |
| Religion | ||
| Christianity | 196 | 96.1 |
| Islam | 8 | 3.9 |
| Duration of service (years) | ||
| < 10 | 54 | 26.47 |
| > 10-20 | 65 | 31.86 |
| > 20-30 | 76 | 37.26 |
| > 30 | 9 | 4.41 |
| Engaging in leisure activities | ||
| No | 51 | 25 |
| Yes | 153 | 75 |
Prevalence of LBP
This study determined the prevalence of LBP to be 70.1%, and the results had been previously published.[18]
Family APGAR and LBP
Most of the participants 188 (92.2%) were from high functioning families, while 16 (7.8%) were from moderately dysfunctional families. None of the respondents were from severely dysfunctional families. Independent t-test showed that there was no significant difference in the family function scores for nurses with LBP and those that did not have LBP (t = 0.716, P = 0.475). Spearman’s correlation did not reveal any significant relationship between severity of back pain and family APGAR scores (Spearman’s r = -0.046, P = 0.606).
Discussion
This study revealed a fairly high prevalence of LBP in keeping with several previous reports.[19] The LBP also had a significant impact on their work ability index as previously reported.[18] Lønnberg et al.[20] in a single general practice in Denmark, had reported that perception of poor working conditions was a far better predictor of long-term outcomes for LBP compared to pain history or clinical features. However, no specific workplace factors were found to be significantly associated with LBP in this cohort of nurses. Hence, this study set out to determine if family factors, specifically family functioning, was a significant contributor to LBP among them.
Almost all the participants were determined to be in highly functional families based on the Family APGAR assessment. This is also in line with similar reports of family functioning among hospital staff in the same environment.[21]
In this study, there was no significant difference in the family function scores for nurses with LBP and those without LBP. This would imply that family functioning as measured by the Family APGAR was not a significant predictor of LBP in nurses.
Limited data is available on the role of family functioning and LBP in nurses. A few studies suggest a causal relationship between poor social relationships outside the immediate work environment and LBP. This relationship is not however consistently demonstrated, as a review by Davis and Heaney[4] found positive associations between poor social relationships and LBP occurring in only about 20% of the studies they reviewed. Baur et al.[22] had reported that work-family conflict is a significant predictor of neck and back pain among surgical nurses in Germany and Switzerland. However, neither social support nor job influence was a statistically significant predictor or modulator of neck or back pain in the same cohort of surgical nurses. It is possible that this complex interplay of factors affecting social support and social relationships, affected our ability to show a relationship between the family functioning and among nurses even when LBP was common.
In a study conducted in South Africa by van Vuuren et al.[5] cultural differences played a role in the perception of family values which might influence the response of individuals indicating their perception of family support. It is possible that this perception of family values and unwillingness to give the true state of family functioning might have influenced the Family APGAR scores determined in our study.
In conclusion, there was a generally high prevalence of LBP among nurses, almost all of whom reported highly functional families. There was no significant difference in the family function scores for nurses with LBP and those without LBP. Further studies with matched cohorts to overcome some of the social confounding variables could be designed in the future to elucidate key family and social predictors of LBP outside the workplace that may affect nurses.
Acknowledgments
The authors wish to acknowledge the assistance of the Nursing Department staff, Jos University Teaching Hospital, Jos, Nigeria.
Financial support and sponsorship
None.
Conflicts of interest
There are no conflicts of interest.
Patient consent
Informed consent was obtained from participants.
Ethics approval
Ethical approval was obtained from the Hospital Research Ethics committee.
REFERENCES
1. Sherching B, Kaswoski W, Marek T. Relationship between risk factors and musculoskeletal disorders in the nursing profession: a systematic review. Occup Ergon 2004;4:241-79.
2. Corona G, Amedei F, Miselli F, Padalino MP, Tibaldi S, Franco G. Association between relational and organizational factors and occurrence of musculoskeletal disease in health personnel. G Ital Med Lav Ergon 2005;27:208-12. (in Italian)
3. Violante FS, Fiori M, Fiorentini C, Risi A, Garagnani G, Bonfiglioli R, Mattioli S. Associations of psychological and individual factors with three different categories of back disorders among nursing staff. J Occup Health 2004;46:100-8.
4. Davis KG, Heaney CA. The relationship between psychosocial work characteristics and low back pain: underlying methodological issues. Clin Biomech (Bristol, Avon) 2000;15:389-406.
5. van Vuuren B, Zinzen E, van Heerden HJ, Becker PJ, Meeusen R. Work and family support systems and the prevalence of lower back problems in a South African steel industry. J Occup Rehabil 2007;17:409-21.
7. Benzon HT, Raja SN, Molby RE, Liu SS, Fishman SM. Essentials of pain medicine and regional anaesthesia. 2nd ed. Philadelphia: Elsevier; 2005. pp. 5-12.
8. Ballantyne J, Fishman SM, Abdi S. The Massachusetts general hospital handbook of pain management. 2nd ed. Philadelphia: Lippincott Williams and Wilkins; 2002. pp. 58-61.
9. Gridley L, van den Dolder PA. The percentage improvement in pain scale as a measure of physiotherapy treatment effects. Aust J Physiother 2001;47:133-8.
10. Hadjistavropoulos T, Herr K, Turk DC, Fine PG, Dworkin RH, Helme R, Jackson K, Parmelee PA, Rudy TE, Lynn Beattie B, Chibnall JT, Craig KD, Ferrell B, Ferrell B, Fillingim RB, Gagliese L, Gallagher R, Gibson SJ, Harrison EL, Katz B, Keefe FJ, Lieber SJ, Lussier D, Schmader KE, Tait RC, Weiner DK, Williams J. An interdisciplinary expert consensus statement on assessment of pain in older persons. Clin J Pain 2007;23:1-43.
11. Jelsma JM. The validity of the Shona version of the EQ-5D, of life measure. S Afr J Physiother 2002;58:8-12.
12. Olaogun MOB, Adedoyin RA, Anitaloba RO. Reliability and concurrent validity of the visual analogue scale and modified verbal rating scale of pain assessment in adult patients with knee osteoarthritis in Nigeria. S Afr J Physiother 2003;59:12-5.
13. Moffet J, Mclean S. The role of physiotherapy in the management of non-specific back pain and neck pain. Rheumatology (Oxford) 2006;45:371-8.
14. Wong DL, Baker CM. Pain in children: comparison of assessment scales. Pediatr Nurs 1988;14:9-17.
15. Kim EJ, Buschman MT. Reliability and validity of the faces pain scale with older adults. Int J Nurs Stud 2006;43:447-56.
16. Cote C, Lerman J, Todres ID. A practice of anesthesia for infants and children. 4th ed. Philadelphia: Elsevier; 2009. pp. 940-65.
17. Araoye MO. "Sample size determination," in research methodology with statistics for health and social sciences. Nathadex: Ilorin, Nigeria; 2004. pp. 115-22.
18. Iyaoromi OO, Madaki AJ, Dankyau M. Relationship between low back pain and work-place functioning of nurses at a tertiary hospital in North Central Nigeria. Internet J Healthc Administr 2016;11:1-7.
19. Sikiru L, Shmaila H. Prevalence and risk factors for LBP among nurses in Africa: Nigeria and Ethiopian specialized hospital survey study. East Afr J Public Health 2009;6:22-5.
20. Lønnberg F, Pedersen PA, Siersma V. Early predictors of the long-term outcome of low back pain--results of a 22-year prospective cohort study. Fam Pract 2010;27:609-14.
21. Dankyau M, Shu'aibu JA, Oyebanji AE, Mamven O, Chima GA. Family functioning of staff of an urban hospital in Nigeria. Internet J Fam Pract 2016;14:1-6.
22. Baur H, Grebner S, Blasimann A, Hirschmüller A, Kubosch EJ, Elfering A. Work-family conflict and neck and back pain in surgical nurses. Int J Occup Saf Ergon 2016;22:1-23.
Cite This Article
Export citation file: BibTeX | RIS
OAE Style
Iyaoromi OO, Dankyau M, Madaki AJK. Relationship between family function and low back pain in nurses working in a tertiary hospital in North Central Nigeria. J Unexplored Med Data 2017;2:16-9. http://dx.doi.org/10.20517/2572-8180.2016.09
AMA Style
Iyaoromi OO, Dankyau M, Madaki AJK. Relationship between family function and low back pain in nurses working in a tertiary hospital in North Central Nigeria. Journal of Unexplored Medical Data. 2017; 2: 16-9. http://dx.doi.org/10.20517/2572-8180.2016.09
Chicago/Turabian Style
Iyaoromi, Omowumi Olamide, Musa Dankyau, Aboi Jeremiah Kutak Madaki. 2017. "Relationship between family function and low back pain in nurses working in a tertiary hospital in North Central Nigeria" Journal of Unexplored Medical Data. 2: 16-9. http://dx.doi.org/10.20517/2572-8180.2016.09
ACS Style
Iyaoromi, OO.; Dankyau M.; Madaki AJK. Relationship between family function and low back pain in nurses working in a tertiary hospital in North Central Nigeria. J. Unexplored. Med. Data. 2017, 2, 16-9. http://dx.doi.org/10.20517/2572-8180.2016.09
About This Article
Copyright

Data & Comments
Data
0

 Cite This Article 1 clicks
Cite This Article 1 clicks

 Like This Article 0
likes
Like This Article 0
likes






Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at support@oaepublish.com.